
Guest contribution:
 Article series on the subject of state-of-the-art mycology in dermatology,
Article series on the subject of state-of-the-art mycology in dermatology,
2nd article

by Prof Hans-Jürgen Tietz, Director of the Institute of Fungal Diseases in Berlin, Germany
Professor Seebacher, a leading dermatomycologist, always warned us never to end onychomycosis therapy too early. Here are the reasons: Mycosis does not confer immunity. But, above all, fungi produce spores in the tissue, which are resistant to laser. However, they are only seemingly dead because they still contain the viable DNA of the pathogen and germinate into virulent hyphae under favourable conditions, causing an endogenous relapse. This often frustrates therapists and patients alike: “Oh bummer! It’s back!”
This also happened with one of our young patients. The whole family was disappointed. Several local pretreatments had been unsuccessful as well as the many cultures, which had not produced a result. Even psoriasis had been suspected, which is hardly treatable. The boy was suffering very much; everyone could see his ugly thumb.
We also failed to grow a culture. It was already negative on the fourth day of local therapy, even though this does not signify a healing success. In order to detect the pathogen in culture we recommend a therapy break in topical pretreatment of four and in systemic therapy of eight weeks before the appointment. However, this is no guarantee for a successful culture. The boy’s family naturally ran out of patience and asked us to perform a PCR, a method that is now well-known from corona testing. A fast and precise result was wanted. The boy had also been pretreated unsuccessfully with terbinafine.
The EUROArray Dermatomycosis PCR showed a result quickly and clearly: T. rubrum. Like every gene test, it can also be performed under therapy, independent of the cultural vitality of the pathogen. A further big advantage of PCR is that it also allows detection of spore DNA. This is hardly possible with conventional methods, apart from searching for spores under the microscope, which is time-consuming and not well remunerated. However, detection of the spores is important, which brings us back to Professor Seebacher and the question of the best time point for ending a therapy. This could previously only be determined microbiologically by means of microscopy. But spores are easy to overlook! Many relapsing patients came back into the practice discouraged. Even the clinical eye can be deceived.
What can we learn from this story? Today, PCR is a useful tool not only for diagnostics but also for therapy monitoring. For the first time, the success of a therapy and thus its termination can be indicated microbiologically in an objective manner – very much in the spirit of Professor Seebacher. A negative PCR result signifies that spore DNA is no longer present and that a relapse of onychomycosis at least in this particular way is excluded. This probably also applied to the presented case.
In this patient the PCR was negative five months following the start of therapy. The thumb nail had healed both clinically and microbiologically. The terbinafine treatment was stopped. It has the potential to cause nail psoriasis as well as a resistance in dermatophytes such as T. rubrum. What a good story, which has become an everyday occurrence thanks to the novel diagnostic (PCR) and therapeutic possibilities.
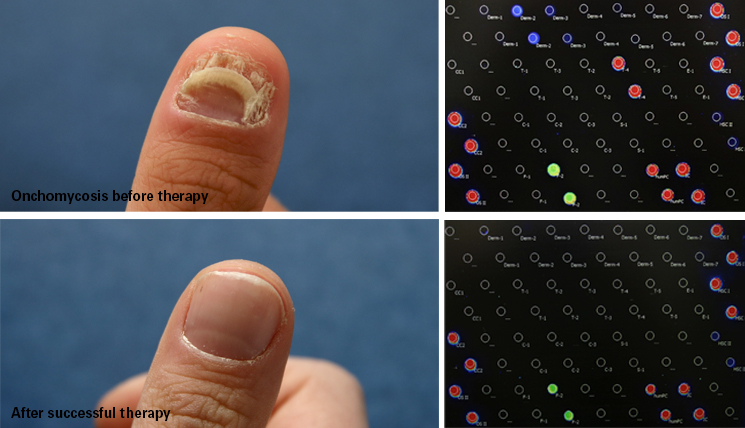
See title image: Onychomycosis in an 8-year old boy, before (A) and after therapy (B) with itraconazole (Itraisdin®) 100mg, daily on days 1-3, plus local urea therapy, based on gene diagnostics (C, T. rubrum) and therapy monitoring (D, negative, at the end of therapy, using the EUROArray Dermatomycosis.
The articles under the rubric “Guest contribution” only reflect the views of the respective authors. Responsibility for the legality and content of the articles lies solely with the authors. EUROIMMUN does not assume liability for the completeness, accuracy and currentness of the information provided.
